

Introduction
Premature Ventricular Complexes – PVCs (aka ventricular ectopic beats – VEBs) are a common, and usually (but not always) benign cardiac rhythm abnormality.
PVCs may present with palpitations, although many cases are asymptomatic.
- Palpitations are often intermittent and brief
- May cause a great deal of anxiety for patients
Beware of patients with syncopal episodes or palpitations (or syncope) associated with exercise.
Most patients can be managed with simple reassurance. Beta-blockers, or calcium channel blockers (second line) can reduced symptomatic episodes.
Terminology
There are a lot of names for the same condition:
- PVC = VEB = ventricular ectopic = ventricular extrasystole
- Bigeminy – refers to a scenario where every normal contraction is followed by a PVC
- Trigeminy – every 3rd contraction is a PVC
- Couplet – two PVC consecutively
- Non-sustained Ventricular Tachycardia – NSVT – 3 or more consecutive PVCs
Pathology
A PVC is an electrical stimulus of the ventricles which occurs within the ventricles themselves – i.e. it does not come from the atria.
- They originate from an ‘ectopic’ (i.e. not the usual place) location in the ventricles
- Caused by groups of pacemaker cells throughout the conduction system that start to operate independently of the normal stimulation
- They can be classified as:
- Unifocal – every PVC appears identical – all arise from he same ectopic location
- Multifocal – different PVC morphologies – indicated multiple ectopic sites
Other types of ectopic also exist:
- Atrial ectopics
- Junctional ectopics
Causes
- Anxiety
- Hypokalaemia
- Hypomagnesia
- Digoxin toxicity
- Excessive caffeine intake
Diagnosis
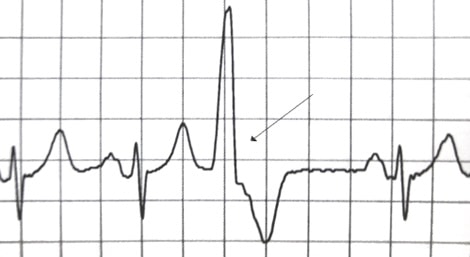
A PVC can be discerned on ECG by:
- Absence of P wave before the QRS
- Wider, taller QRS complex (>120ms)
- Often immediately follows a T wave
- Has a discordant T wave (T wave point in opposite direction to major portion of QRS)
Usually, one or more PVCs will be visible on an ECG – even if the patient is asymptomatic at the time of presentation
- Consider 24-hour ECG (Holter Monitor) if normal ECG at the time of presentation

Management
- Rule out structural heart disease with an echo
- If present – refer to cardiology
- Assess for risk of acute cardiac mortality
- FHx of sudden cardiac death
- Previous history of syncope?
- Especially if associated with exercise
- Increase in palpitations after exercise
- If all the above is normal:
- Reassure
- Consider beta-blocker or calcium-channel blocker
- Hotly debated whether or not caffeine cessation helps to reduce PVCs and / or symptoms
References
- Premature Ventricular Complex (PVC)
- Murtagh’s General Practice. 6th Ed. (2015) John Murtagh, Jill Rosenblatt
- Oxford Handbook of General Practice. 3rd Ed. (2010) Simon, C., Everitt, H., van Drop, F.
- Beers, MH., Porter RS., Jones, TV., Kaplan JL., Berkwits, M. The Merck Manual of Diagnosis and Therapy


